房间隔封堵器封堵支气管胸膜瘘1例报告
张 莉 叶联华 王高伟 张 磊 陈 雅 谭 慧▲黄云超
云南省肿瘤医院胸外一科 云南省肺癌研究重点实验室,云南昆明 650118
[摘要]支气管胸膜瘘是肺切除术后罕见但最严重的并发症之一,病死率高。有效的治疗方法对支气管胸膜瘘的预后有重要意义。目前对于支气管胸膜瘘的治疗尚无相关指南和标准,为评估房间隔封堵器封堵全肺切除术后早期支气管胸膜瘘(BPF)的临床疗效,本文回顾性分析2016年12月云南省肿瘤医院胸外一科诊治的1例临床诊断为左全肺切除术后支气管胸膜瘘患者的临床资料。该患者临床表现为咳嗽,咳痰,伴痰中带血,复查胸部CT和电子支气管镜,发现左肺支气管胸膜瘘。根据支气管胸膜瘘的解剖特点和病变特征,采用房间隔封堵器封堵瘘口。第1次置入房间隔封堵器(6 mm)时,一次置入成功,房间隔封堵器置入后左肺支气管瘘口完全封堵。5 d后做电子支气管镜检查,评估肺部和气道情况,发现左肺支气管残端封堵器移位。再次置入房间隔封堵器(18 mm),一次置入成功,瘘口完全封堵。封堵器置入3个月后患者左侧胸膜残腔完全消失,瘘口愈合,肺功能明显改善。应用房间隔封堵器对肺叶切除术后形成的早期支气管胸膜瘘进行封堵,操作简单,加快瘘口愈合,残腔消失。改善患者的生活质量,临床效果良好。通过临床资料分析,房间隔封堵器封堵支气管胸膜瘘是一种科学有效、瘘口愈合快、手术安全性好、操作简便、术后并发症少的治疗新方法,可推广应用。
[关键词]肺切除术;支气管胸膜瘘;房间隔封堵器;电子支气管镜
支气管胸膜瘘(bronchopleural fistula,BPF)是指支气管残端与胸膜腔形成的瘘道,据相关文献统计,支气管胸膜瘘的发生率为0.5%~15.0%,但是其病死率却高达23.6%~71.2%[1]。有学者提出房间隔封堵器封堵支气管胸膜瘘具有简便、安全、有效等优点[2]。支气管胸膜瘘可由多种原因引起,如支气管残端闭合技术、残端有癌残留、胸腔感染、某些全身性疾病(如糖尿病、低蛋白血症、免疫缺陷、营养不良等)、术前辅助放疗或化疗、术后机械通气>24 h及术后感染等[3-4]。支气管胸膜瘘是肺切除术中罕见但可能致命的并发症[5]。云南省肿瘤医院胸外一科诊治了1例左下肺鳞癌的患者,行左全肺切除术后发生左主支气管残端胸膜瘘,两次置入房间隔封堵器后,封堵完全,治疗效果好,现报道如下。
1 病例资料
患者,男,65岁,因左肺鳞癌于2016年12月24日行左全肺切除术,手术成功,顺利出院。3 d后因咳嗽、咳痰,痰中带血再次入院,复查CT提示:左侧支气管残端-胸膜瘘形成,内、外口径约0.26 cm。放置胸腔闭式引流管,咳嗽时有气泡溢出,首次置入房间隔封堵器(6 mm)后,封堵良好。5 d后患者咳嗽时胸管内仍有气泡溢出,复查电子支气管镜,提示左侧支气管残端封堵器下移,窥见瘘口。考虑首次置入房间隔封堵器型号(6 mm)不适宜该瘘口大小,更换为房间隔封堵器(18 mm)(图 1),置入后封堵完全(图 2),患者咳嗽时无气泡溢出,考虑封堵器置入有效,封堵完全。

图1 房间隔封堵器
术前行胸部横断位及支气管成像,测量左主支气管的残端和直径,采用房间隔封堵器18 mm
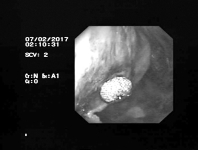
图2 支气管镜下所示
术中置入房间隔封堵器(18 mm)完全封堵住左肺支气管残端胸膜瘘口
患者全麻后气管插管,电子支气管镜通过气管插管依次进入气管、隆突、右主支气管及各段支气管,未见明显异常,吸出较多黏性分泌物;观察发现左肺支气管残端封堵器移位,窥见瘘口大小约12 mm,之前所用封堵器脱落,于是将其取出,将房间隔缺损封堵器(18 mm)用封堵器介入输送装置(8 f)送入胸膜腔,封堵器成型好,内镜下未见残余瘘,释放整个封堵器,术中顺利。持续放置胸腔闭式引流管引流,3 d后患者恢复良好出院。
2 讨论
目前,肺切除术后导致的支气管胸膜瘘仍然是非常棘手的问题。现在的治疗方式有以下3种:①外科手术治疗。再次手术关闭瘘口、闭式引流或开窗引流治疗对全肺切除术后支气管胸膜瘘患者具有较好的效果[6]。此外采用带蒂肌瓣也可以获得良好的治疗效果[7-9]。但外科手术治疗创伤性大,患者耐受性差,易复发,远期疗效不确切,上述外科手术方式未获得广泛应用[10]。②介入封堵治疗。主要包括纤维支气管镜下“三明治”疗法[11]、瘘口<5 mm用封堵剂直接封堵、气管镜下注入硬化剂[12]、瘘口下插入PVA海绵和氰基丙烯酸酯胶[13]、局部热疗刺激肉芽增殖等治疗,瘘口>5 mm时置入支气管封堵器[14]、气道支架及房间隔缺损封堵器[2]等治疗,气管镜下治疗具有创伤性小、患者耐受性好、可反复多次巩固治疗等优点,治疗效果好[10]。全覆膜自膨式金属支架对一侧肺叶切除术后的支气管胸膜瘘患者具有较好疗效[15]。③骨髓间充质干细胞对支气管胸膜瘘封堵成功[1,16]。
本例报道中,该患者两次行封堵术,封堵器均一次成功置入,手术顺利。首次封堵器置入5 d后发生移位可能是由于肺部感染导致瘘口与封堵器贴合不严密,封堵器狭部稍大于瘘口内径,一定程度上扩张了瘘口直径,而第二次术前及术后给予积极的抗感染治疗,胸腔闭式引流管冲洗胸腔,房间隔缺损封堵器型号较大,贴合较好,封堵完全。实践证明该封堵器及其置入系统使用方便,易于定位,封堵效果确切,组织相容性好,未发生封堵器移位和脱落现象。
综上所述,房间隔缺损封堵器及其置入系统是一种安全、有效且使用方便的支气管胸膜瘘内封堵的器材,应用房间隔封堵器对肺叶切除后形成的支气管胸膜瘘进行封堵,临床效果良好,可推广应用。
[参考文献]
[1]宋亚亚,高宝安.骨髓间充质干细胞在支气管胸膜瘘中的研究进展[J].实用医学杂志,2015,31(15):2581-2582.
[2]王洪武,张楠,李冬妹,等.房间隔封堵器治疗支气管残端胸腔瘘二例效果分析[J].中华结核和呼吸杂志,2017,40(4):314-315.
[3]冯竞,刘晓芯,朱渊.一例左全肺切除术后并发支气管胸膜瘘及右肺严重感染的护理[J].护士进修杂志,2015,30(22):2110-2111.
[4]Okuda M,Go T,Yokomise H.Risk factor of bronchopleural fistula after general thoracic surgery:review article[J].Gen Thorac Cardiovasc surg,2017,65(12):679-685.
[5]Nachira D,Chiappetta M,Fuso L,et al.Analysis of risk factors in the development of bronchopleural fistula after major anatomic lung resection:experience of a single centre[J].ANZ J Sur,2017,(10):1111.
[6]李洋,栾颖,崔有斌,等.全肺切除术后早期支气管胸膜瘘的治疗[J].中华医学杂志,2016,96(21):1692-1695.
[7]Elswick SM,Sharaf B,Hammoudeh ZS,et al.Endobronchial-Guided Vascularized Tissue Flaps for a Bronchopleural Fistula[J].Ann Thorac Surg,2017,104(1):e1-e3.
[8]张勇,冯自豪,杨燕文,等.带蒂肌瓣胸腔内转移填塞治疗脓胸创面[J].中华整形外科杂志,2014,30(6):428-431.
[9]Fricke A,Bannasch H,Klein HF,et al.Pedicled and free flaps for intrathoracic fistula management[J].Eur J Cardio thoracic surg,2017,52(6):1211-1217.
[10]唐飞,程超,吕莉萍.应用利福霉素定位支气管胸膜瘘并封堵 1 例[J].中国内镜杂志,2017,23(5):108-110.
[11]卢春来,袁云锋,葛棣,等.纤维支气管镜下“三明治”疗法治疗肺手术后支气管胸膜瘘(BPF)[J].复旦学报(医学版),2015,42(2):187-190.
[12]李洋,张逸远,崔有斌,等.经支气管镜注射硬化剂治疗支气管胸膜瘘22例临床分析[J].中华外科杂志,2017,55(7):554-555.
[13]Battistoni P,Caterino U,Batzella S,et al.The use of polyvinyl alcohol sponge and cyanoacrylate glue in the treatment of large and chronic bronchopleural fistulae following lung cancer resection[J].Respiration,2017,94(1):58-61.
[14]丁培堃.介入封堵治疗肺切除术后支气管胸膜瘘的研究进展[J].中国微创外科杂志,2017,17(8):728-731.
[15]Cao M,Zhu Q,Wang W,et al.Clinical application of fully covered self-expandable metal stents in the treatment of bronchial fistula[J].Thorac Cardiovascr Surg,2016,64(6):533-539.
[16]Aho JM,Dietz AB,Radel DJ,et al.Closure of a recurrent bronchopleural fistula using a matrix seeded with patientderived mesenchymal stem Cells[J].Stem Cells Transl Med,2016,5(10):1375-1379.
A report about bronchopleural fistula after the treatment of atrial septal defect occluder
ZHANG LiYE Lian-huaWANG Gao-weiZHANG LeiCHEN YaTAN Hui▲HUANG Yun-chao
The First Department of Thoracic Surgery,Yunnan Cancer Hospital,Key laboratory of lung cancer research in Yunnan province,Kunming 650118,China
The First Department of Thoracic Surgery,Yunnan Cancer Hospital,Key laboratory of lung cancer research in Yunnan province,Kunming 650118,China
[Abstract]Bronchopleural fistula is one of the most rare but serious complications after pneumonectomy,with high mortality.Effective treatment is of great significance to the prognosis of bronchopleural fistula.At present,there are no relevant guidelines and standards for the treatment of bronchopleural fistula.In order to evaluate the clinical efficacy of atrial septal occluder for early bronchopleural fistula(BPF)after total pneumonectomy,this paper retrospectively analyzed the clinical data of one case diagnosed as bronchopleural fistula after total pneumonectomy in Yunnan cancer hospital in December 2016.The clinical manifestations of this patient are cough,expectoration,accompanied by blood in sputum,did chest CT and electronic bronchoscopy,then found left pulmonary bronchopleural fistula.According to the anatomical characteristics and pathological features of bronchopleural fistula,the atrial septal occluder was used to occlude the fistula.The first placement of the atrial septal occluder(6 mm)was successful,and the left pulmonary bronchial fistula was completely occluded after placement of the atrial septal occluder.Five days later,an electronic bronchoscopy was performed to assess the pulmonary and airway conditions and found that the left pulmonary bronchial stump occluder was displaced.To place the atrial septal occluder(18 mm)again,once placed successfully,and the fistula was completely occluded.The left pleural residual cavity disappeared completely after the occluder was placed for 3 months,the fistula healed and the pulmonary function improved obviously.The atrial septal occluder was used to occlude the early bronchopleural fistula after lobectomy.The operation was simple,the fistula healing was accelerated and the residual cavity disappeared.As well as improve the quality of life of patients,the clinical effect is good.A large number of clinical data shows that the atrial septal occluder is a scientific and effective method which owes the advantages of the treatment of bronchopleural fistula,rapid healing of fistula,good surgical safety,simple and convenient operation and less postoperative complications.It can be popularized and applied.
[Key words]Pneumonectomy;Bronchopleural fistula;Atrial septal defect occluder;Electronic bronchoscope
[中图分类号]R541.1
[文献标识码]A
[文章编号]1674-4721(2018)2(c)-0145-03
[基金项目]云南省卫生科技计划项目(2016NS108)
[作者简介]张莉(1994-),女,云南宣威市人,2017 级在读硕士研究生,研究方向:呼吸内镜介入诊治
▲通讯作者:谭慧(1971-),女,硕士,主任医师,研究方向:呼吸内镜介入诊治
(收稿日期:2017-11-14 本文编辑:闫 佩)